Diabetic Foot Checks at Home for Families
Diabetic foot care at home works best when daily checks are simple, visible, and easy for families to repeat. Photo source
The practical search query this article answers is diabetic foot care at home. It is for the person with diabetes who wants to keep their feet safe, and for the family member or carer who is worried about nails, hard skin, shoes, swelling, or a small mark that was not there last week.
Why diabetes changes ordinary foot care
Diabetes can make foot problems easier to miss and slower to heal. Foot guidance explains that long periods of high blood glucose can damage nerves in the feet, and circulation can also be affected by factors such as blood pressure, cholesterol, smoking, heart disease, or stroke. That is why a small rub, blister, crack, or nail edge may matter more when someone has diabetes than it would for another person.
The important point is not to become frightened of every normal foot change. It is to have a routine. People with diabetes should have their feet checked when diabetes is diagnosed and at least once a year after that, and the check includes skin, hard skin, infection, shape, footwear, feeling, and blood flow. Home care should support that professional review, not replace it.
This is where home care becomes practical rather than abstract. The person may not be able to reach their feet, may not travel easily, or may need a steady routine between annual checks. A good home routine keeps small changes visible and helps families know when routine foot care is enough and when medical advice is needed.
What to check every day at home

Daily checks should be simple enough to repeat, especially when a family member or carer is helping. Photo source
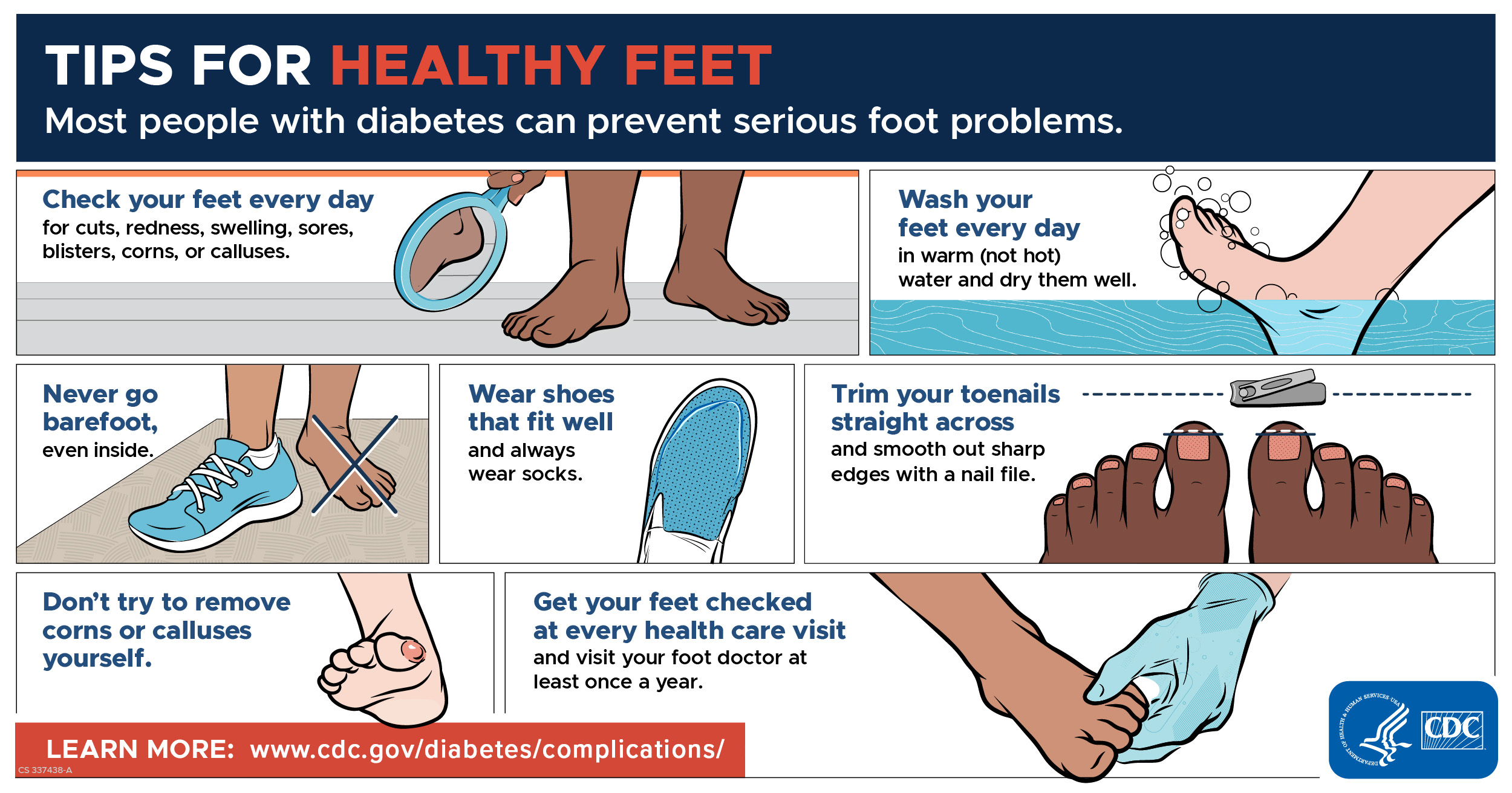
The best home routine is short and consistent. Look at the tops, soles, heels, sides, toenails, and between the toes. Use a mirror if bending is difficult, or ask a trusted person to help. NHS diabetic foot guidance recommends looking daily for cuts, skin breaks, hard skin, swelling, heat, shape change, or new pain.
For carers, the check can often happen during normal personal care rather than as a separate medical event. Carer guidance for diabetic foot care says carers should check feet regularly when supporting personal care, and refer on for red areas, inflammation, blisters, corns, callus, or open areas. That is practical because the person may not feel pain clearly if sensation is reduced.
A simple phrase helps: look, feel, compare. Look for marks, cracks, bruises, hard skin, nail pressure, redness, swelling, or discharge. Feel whether one foot is warmer, colder, more swollen, or more tender than usual. Compare with yesterday or last week. Nursing foot check guidance uses an ask, look, and feel approach, including questions about new colour, shape, temperature, pain, blisters, cuts, cracks, or nail problems.
Nails, corns, and hard skin need caution
Many families search because one specific task has become difficult: cutting toenails, dealing with hard skin, or trying to reduce a corn. With diabetes, the safest rule is to avoid digging, cutting down the sides of nails, using sharp blades, or trying to remove corns and calluses yourself. The CDC's foot care checklist says people with diabetes should not try to remove corns or calluses themselves.
That does not mean routine care should be delayed. It means the right person should do the right part of the job. If nails are long, thick, curved, painful, or pressing into skin, a home visit can help with careful trimming and advice. If hard skin is building or a corn is painful, the focus should be pressure relief and safe treatment rather than bathroom surgery.
The Royal College of Podiatry points people with diabetes toward approved foot care information leaflets developed with national diabetes and podiatry organisations, which is a useful reminder that diabetic foot care is a risk management habit, not just cosmetic maintenance. For routine home care, the safest pattern is gentle washing, thorough drying, moisturising away from the toes, suitable footwear, and professional advice when the foot is higher risk.
Footwear and socks are part of the care plan
A good foot care routine includes checking shoes, slippers, socks, and pressure points, not just the skin. Photo source
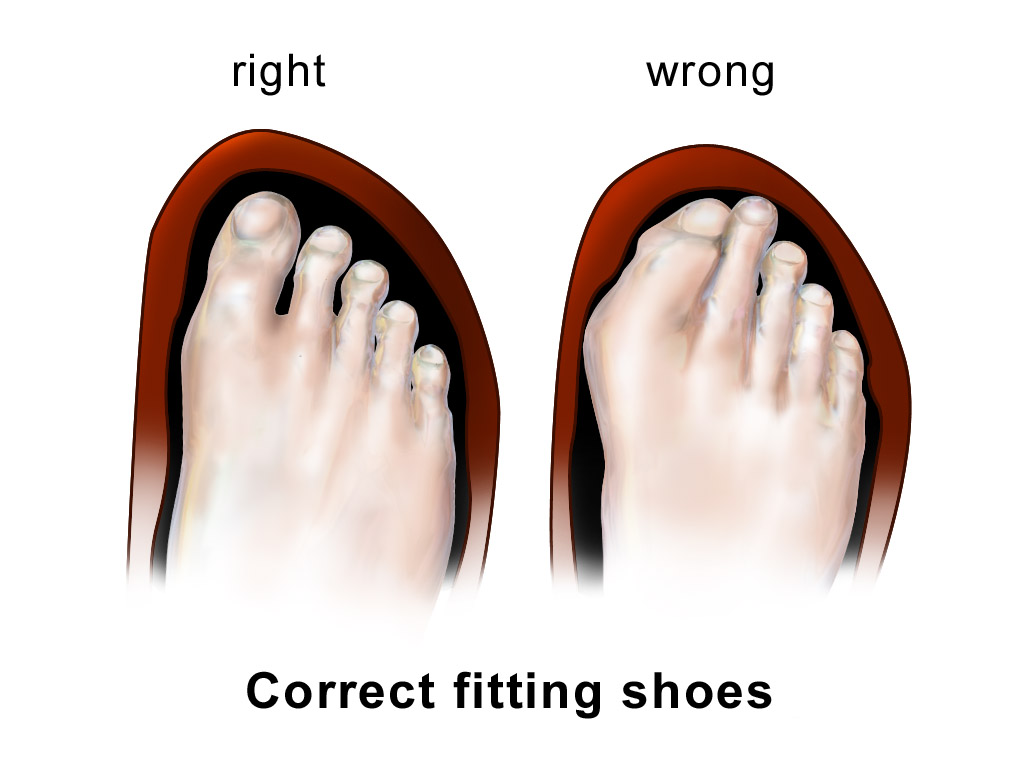
Shoes and slippers can quietly cause problems. A seam, tight toe box, loose heel, worn insole, or curled sock can keep rubbing the same place. Patient guidance on looking after diabetic feet recommends footwear that is wide fitting, has a deep toe area, is flat or low heeled, fastens securely, and is not too tight or too loose. It also suggests light coloured socks to make bleeding or fluid easier to spot.
At home, this means checking the inside of shoes before they go on, changing socks daily, avoiding bare feet, and watching whether a certain pair of slippers causes the same red mark. Older people may also have swelling, balance issues, stiffness, or a changed walking pattern. Parkinson's foot care guidance notes that gait changes, stiffness, swelling, and balance issues can affect feet and footwear, including shoe fit and pressure problems.
This is one reason home visits can be useful. The shoes, socks, chair, bathroom routine, lighting, and walking route are all there. Advice can be tied to what the person actually wears and does, rather than a clinic conversation that depends on memory.
When a foot problem needs urgent advice
Some changes should not wait for a routine appointment. Seek urgent advice if there is a hot, red, swollen foot, new skin damage, a new wound, discharge, spreading redness, sudden swelling, a change in foot shape, new pain, fever, shivering, nausea, or feeling generally unwell. NHS inform advises urgent contact with a podiatrist or GP for a hot red swollen foot, new skin damage, shape change, or new pain, and 111 if new foot issues come with feeling unwell.
Clinical pathway guidance treats new ulceration, swelling, discolouration, infection, acute pain, or possible Charcot changes as red flags. It also says suspected urgent diabetic foot problems should be seen quickly by the appropriate foot team. In plain English, new swelling, colour change, infection, ulceration, or unexplained acute pain should not be treated as normal nail care.
A risk chart based on NICE guidance separates low risk, moderate risk, high risk, active foot disease, and foot emergencies. It describes active disease as ulceration or an unexplained hot red swollen foot, and says active foot problems need prompt specialist triage. That matters at home because a family member may see the change first. If the foot has moved beyond routine care, the next step is medical assessment, not more home trimming.
Why home visits help families and carers
Home visit foot care is most helpful when the barrier is practical. The person may be older, anxious about travelling, unable to bend safely, housebound, recovering from illness, or relying on a carer to arrange everything. Age UK notes that foot care services for older people may be accessed at home if someone is housebound, and that good foot care can relieve pain and reduce the risk of infection and falls.
For families, the difficulty is often knowing where foot care ends and wider support begins. Carers UK describes how arranging support for someone can feel hard at the start, especially when you are trying to make an informed choice in their best interests. A foot care visit can solve a focused problem, while still leaving room for GP, podiatry, social care, or district nursing support when the foot risk is higher.
For RMFC patients in Surrey, the commercial fit is clear but should stay calm. If the need is routine comfort, careful nail care, callus support, footwear pressure advice, or help because clinic travel is difficult, a diabetic foot care home visit may be appropriate. If there is an open wound, sudden swelling, infection, or a hot red foot, the safer route is urgent medical advice first.
How to prepare for a diabetic foot care home visit
Preparation should be simple. Choose a well lit room, have a comfortable chair ready, keep the shoes and slippers that are worn most often nearby, and mention diabetes, circulation problems, numbness, previous ulcers, blood thinning medication, allergies, recent infections, and any new pain or skin change before treatment begins.
It helps to write down what changed and when. For example: "right heel crack noticed on Monday", "left big toenail pressing in shoe", "new red mark after wearing slippers", or "cannot feel the toes as clearly". Diabetes in Grampian advises daily foot checks and says that if you discover breaks in the skin, minor cuts, or blisters, you should cover the area and contact the local podiatry service for further advice.
A home visit can then focus on the right goal: safe routine care when it is appropriate, and clear signposting when the foot needs GP, NHS podiatry, or urgent assessment. If the problem is routine but difficult to manage alone, asking about a home visit is a practical next step.
Key Takeaways
- Diabetic foot care at home is about daily checks, safe routines, and knowing when to ask for help.
- Look for new cuts, cracks, blisters, hard skin, swelling, heat, redness, shape change, or new pain.
- Do not cut corns, dig at callus, or keep trimming painful nails when diabetes or reduced feeling is involved.
- Shoes, slippers, socks, and pressure points are part of the care plan.
- A home visit can help with routine care, but wounds, infection, sudden swelling, or a hot red foot need medical advice.
Diabetic foot care at home should feel steady rather than scary. A daily check, sensible footwear, careful nail and skin care, and early action on changes can make a real difference. For families in Surrey, RMFC can help when routine foot care is difficult to manage or travel is a barrier, while keeping the boundary clear when a diabetic foot problem needs medical assessment first.
Need Professional Foot Care?
Book a home visit and get expert treatment without leaving your house